Surgical hand disinfection

Preoperative rub-in procedure by the application of a hand disinfectant before donning surgical gloves. Aims at the hands' microbial flora...
Learn more

Surgical site infections (SSI), infections that occur after surgeries, can be superficial or involve deeper tissues, organs, or implanted materials. They are most frequently caused by pathogenic bacteria, less often by viruses or fungi. Which pathogens cause SSI is generally dependent on the performed procedure [1, 2]. For example, facultative pathogens only become problematic in combination with other factors such as the insertion of an implant [1].
This overview provides information on the most important bacterial pathogens for SSI.
In Germany the most common pathogen causing SSI is S. aureus [1]. Data collected by the National Reference Center for Nosocomial Infections (Nationales Referenzzentrum für nosokomiale Infektionen, NRZ) in the hospital infection surveillance system ‘KISS’ show that S. aureus can be found in 20% of all SSI isolates [1]. Also, in data from the US, captured in the National Healthcare Safety Network (NHSN) of the Centers for Disease Control and Prevention (CDC), S. aureus was identified in 20.7% of all SSI cases [2]. SSI with S. aureus are particularly frequent after cardiac and orthopaedic surgeries [1]. One major risk factor is nasal colonisation of the patient with S. aureus, which can be tackled by preoperative screening and decolonisation [1].
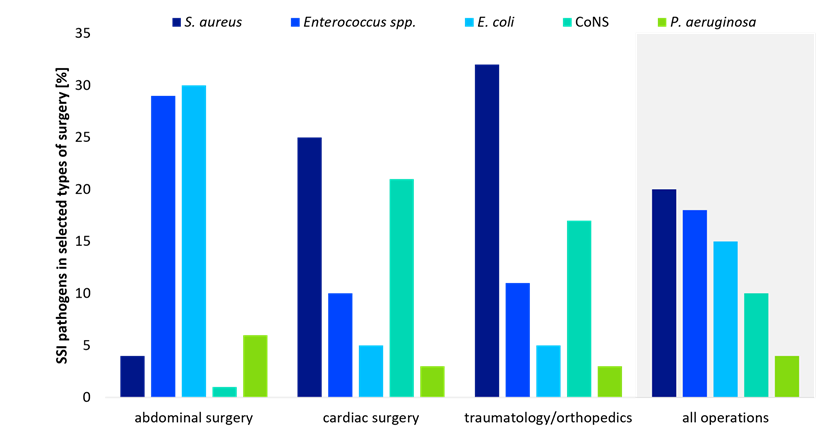
In abdominal surgery, on the other hand, intestinal bacteria play a particularly important role for SSI. Here, E. coli is the leading pathogen with 30% (NRZ) and 19.6% (NHSN) of SSI cases, followed by enterococci (NRZ 29%, NHSN 13.9%) [1, 2]. Preoperative defecation in combination with antibiotics can reduce this risk in certain surgeries [1].
Orthopaedic surgeries carry a particularly high risk of osteomyelitis (bone infection due to spread from surrounding tissue, systemic bacteraemia, or direct bone trauma), which is mostly caused by S. aureus or coagulase-negative Staphylococci from the normal skin flora [3]. Propionibacterium acnesoften causes SSI after shoulder surgeries, because this bacterium preferably colonises the skin of shoulder and axilla [4]. Operations in which foreign materials are introduced (e.g., joint replacements in orthopaedics) are associated with a particularly high risk of SSI. Since the material properties of the implants favour the adhesion of bacteria (biofilm formation) fewer pathogens may be needed to cause an infection. This risk, however, can be mitigated using special materials such as titanium or antiseptic coatings [1].
Depending on the operation, different pathogens play a role in SSI. It is therefore fundamental to implement the hygiene measures recommended in guidelines for preparation of the patient [1, 5]. Since there is a risk of SSI not only from the patient's own flora (endogenous), but also from surfaces, instruments and hands (exogenous), compliance with hygiene measures (e.g., indicated hand, surface and instrument disinfection) is essential to prevent infections and increase patient safety.
Sources:




